Neurocrine Access Support Program Overview
A guide outlining the benefits and services offered through the Neurocrine Access Support Program

Neurocrine Access Support was created to ensure that you have all the information that you, your staff, and your patients need to access INGREZZA capsules or INGREZZA SPRINKLE capsules. We're here to support you every step of the way so that you can focus on what really matters.
Access these resources to help your patients who are prescribed INGREZZA or INGREZZA SPRINKLE capsules.
For assistance creating a customized letter of medical necessity or appeals, ACEHOUND can help simplify the process with intelligent letter templates and guided workflows, visit ACEHOUND.com/INGREZZA
Neurocrine Access Support Program Overview
A guide outlining the benefits and services offered through the Neurocrine Access Support Program
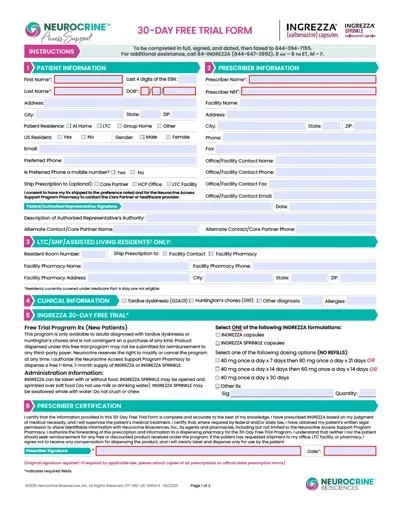
INGREZZA 30-Day Free Trial Form
Enroll eligible patients in the 30-Day Free Trial program for a free 30-day supply of INGREZZA
A free 1-month supply of INGREZZA is available for new patients. Download and fax the completed form to 844-394-7155.*
*The program is not contingent on a purchase of any kind. Product dispensed under this free trial program may not be submitted for reimbursement to any third-party payer. We reserve the right to modify or cancel the program at any time.
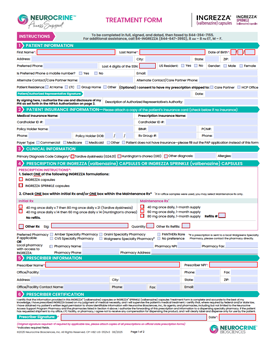
INGREZZA Treatment Form
An all-in-one form to prescribe INGREZZA and enroll eligible patients in the support program
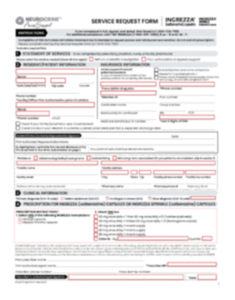
INGREZZA Service Request Form
A form to request a benefit investigation, prior authorization, or reimbursement support. This form can be downloaded and faxed or submitted electronically
CoverMyMeds
Click below to log in to your CoverMyMeds account
ACEHOUND
ACEHOUND can simplify the creation of letters of medical necessity and appeals

Sample Appeal Letter
A customizable template to support coverage appeals with insurance plans on behalf of a patient
Sample Letter of Medical Necessity
A template letter to help demonstrate medical need for INGREZZA therapy for payer approval
Just Say No Flashcard
An overview of the Neurocrine Access Support program and available options if a patient's insurance requires a PA or appeal
Pathway to Successful Medicare Part D Appeals
An overview of the appeals process and helpful tips for successful appeals for Medicare Part D patients
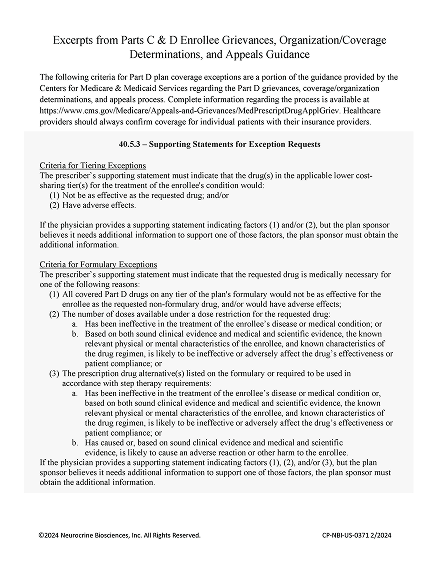
40.5.3 Supporting Statements
Excerpts from Medicare Parts C & D enrollee grievances, organization/coverage determinations, and appeals guidance
Medicare Part D Extra Help Program Information
An overview of financial assistance available through Medicare Part D's Extra Help Program for eligible patients
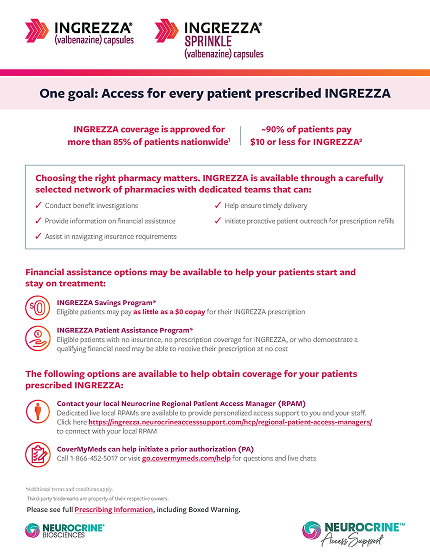
INGREZZA Patient Assistance Program Application
Application form for patients seeking financial support through the INGREZZA Patient Assistance Program

INGREZZA Savings Program
Commercially insured patients may be eligible to pay $0 for their INGREZZA prescription
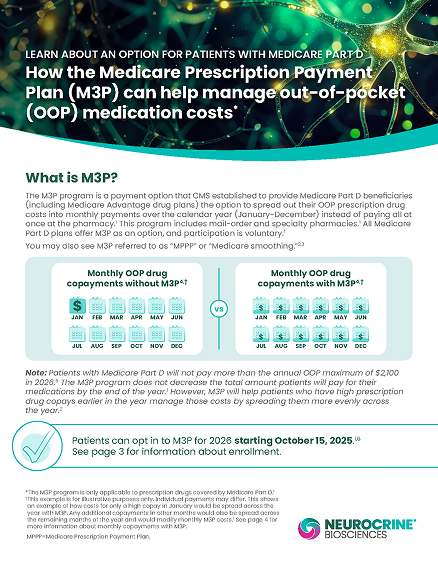
Medicare Prescription Payment Plan (M3P)
An overview of a payment option established by the Centers for Medicare & Medicaid Services to provide Medicare Part D beneficiaries
Third-party trademarks are property of their respective owners.